Annals of Middle Eastern Medicine
Khalid M. Alghuthayr et al. Annals of Middle Eastern Medicine. 2026;2(1):077-084
REVIEW ARTICLE
Examining the relationship between nomophobia and depression: a systematic review and meta analysis of 10 studies involving 12,043 participants
Khalid M. Alghuthayr1*, Rakan H. Hamzah1, Othub S. Albalawi1, Mohammed A. Binjabr1,2, Idrees S. Alalawi1, Fatima A. Hamidaddin1, Saad M. Alotaibi1, Turki M. Alomar1,3, Haitham Jahrami1,4
Correspondence to:Khalid M. Alghuthayr
*Department of Psychiatry, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Bahrain.
Email: Kalghuthayr@gmail.com
Full list of author information is available at the end of the article.
Received: 10 January 2026 | Revised (1): 15 February 2026 | Revised (2): 17 February 2026 | Accepted: 04 March 2026
ABSTRACT
Background:
This comprehensive review investigates the distinct relationship between nomophobia and depression, aiming to isolate their association. While prior research has explored the collective impact of nomophobia on various psychological problems, this study focuses on highlighting the specific effects of nomophobia on depression.
Methods:
A systematic review and meta-analysis were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 statement. Ten studies comprising 12,043 participants were included. A random-effects meta-analysis and linear regression analysis were performed to assess prevalence rates and the association between moderate to severe nomophobia and depression.
Results:
The pooled prevalence of moderate to severe nomophobia was 63.2% (95% CI: 51.00%-73.86%), while 26.2% of participants (95% CI: 19.37%-34.36%) reported depression. Linear regression analysis revealed no direct linear relationship between moderate to severe nomophobia and depression.
Conclusion:
This study suggests that the link between depression and nomophobia is not direct. Nomophobia may be more closely associated with anxiety-related constructs rather than depressive symptomatology.
Keywords:
Systematic review and meta-analysis, nomophobia, smartphones, anxiety disorder, depression, moderate to severe nomophobia.
Introduction
Smartphones have become a household staple in every family and the most standard means of communication [1]; it is no surprise that a plethora of psychological and anxiety disorders emerged along with the excessive use of this technology [2]. Nomophobia is an acronym for No mobile phone phobia [3]. It is a neo-psychological disorder that is defined as the fear of being disconnected from others [4] or of being unable to communicate with other people by utilizing smartphone applications and services [5]. Recent systematic reviews have reported that the prevalence of nomophobia varies widely across populations, with rates frequently exceeding 60%, particularly among university students [6],[7]. These findings highlight the growing global concern regarding excessive smartphone dependence.
Nomophobia correlates with a number of psychological problems as well as poor functioning [6],[7]. This condition is associated with insomnia and other sleep problems [8],[9], symptoms of depression [10], anger issues [11], stress and anxiety disorders [4],[6],[10], hyperactivity, and defiance [11], low self-esteem [12], poor quality of life [5],[10], and below-average academic performance [13]-[15].
Depression and dysthymia, substance use disorders, anxiety and social anxiety disorders, obsessivecompulsive disorder, eating disorders, and other behavioral addiction disorders have been reported to be comorbid with nomophobia [10]. Depressed adolescents will likely seek social media to help them cope with feeling lonely and to feel better about themselves [10]. Conversely, it may also be likely that symptoms of depression are aggravated by the perception that the lives of other individuals are more fulfilling than their own, as portrayed in social applications [10].
Several papers have studied the collective association of nomophobia with depression along with other psychological problems; however, few papers have isolated the association of nomophobia with depression. For this reason, in the present study, we aim to highlight the effects of nomophobia on depression and to examine whether an independent association exists on its own, or if it was merely a coincidental correlation in previous literature [10],[16].
Materials and Methods
This systematic review and meta-analysis were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement [17].
Information sources and search strategy
In accordance with the PICO framework, an electronic search of the literature was performed independently by two members on multiple databases, including Scopus, ScienceDirect, Pubmed/MEDLINE, PsycINFO, and the Web of Science. Using Boolean operators (OR, AND) to combine searches, we combined the terms “nomophobia” or “no-mo-phobia” or “no mobile phobia” or “mobile phone” or “mobile addiction” and “prevalence” and “depression”. The selected studies were evaluated using full-text copies.
Eligibility criteria
Two authors (OSA and RHH) independently assessed the articles for eligibility. Studies were included if they met the following criteria: (1) English-language published papers from database inception until February 28, 2023; (2) participants aged over 12 years; (3) participants’ responses to each test were scored and reported so that the percentage of participants falling above and below predetermined cutoff points could be calculated; and (4) studies that assessed nomophobia and its association with depression. Studies were excluded if they were: (1) case reports, commentaries, conference abstracts, poster presentations, reviews, or dissertations; or (2) articles inaccessible for full-text review.
Data extraction
After deduplication, three reviewers (MBJ, ISA, and RHH) independently performed data extraction using standardized Microsoft Excel spreadsheets (Microsoft Excel, Microsoft Corporation, Version 365). The following information was collected: author name, publication year, country of data collection, sample size, gender (male/female ratio), and the reported numbers of patients with nomophobia and depression.
Risk of bias assessment
Two investigators (ISA, KMA) independently fulfilled the quality assessment using the Newcastle.Ottawa Scale (NOS) checklist [18]. The quality score ranged between 0 and 9. Study scores of eight or nine points corresponded to high quality with a low risk of bias, five to seven points to moderate quality, and four or fewer points to low quality with high risk of bias.
Results
Descriptive results
The electronic database search identified a total of 10 studies after removing duplicates and automated screening. The selection process described in Figure 1 resulted in 10 qualified studies for this meta-analysis. All included studies were published between 2018 and 2023 and collectively comprised 12,043 participants from six countries. Detailed results are shown in Table 1.
The countries included Brazil (K = 1), the Kingdom of Saudi Arabia (KSA, K = 1), Peru (K = 2), India (K = 4), Lebanon (K = 1), and Germany (K = 1), as K denotes the number of studies per country. The country providing the most studies was India (K = 4, 40%). Figure 2 shows the distribution of the studies worldwide. All the studies used the Nomophobia Questionnaire (NMP-Q) scale to report the prevalence of nomophobia. However, not all the studies used the same scale to assess depression. As Depression Anxiety Stress Scales-21 (DASS-21) is being used in four studies [20],[22],[23],[26], Hopkins Symptom Checklist-25 (HSCL-25) in 2 studies [22],[24], Beck Depression Inventory (BDI) in one study [10], Hamilton Depression Rating Scale (HDRS) in one [8], and two studies [22],[25] did not report what scale they used to assess depression. Figure 2 shows the distribution of the studies worldwide.
The mean number of participants per study was 1,204 (range 145-3,139), and the mean age was 19.7 years (range 16-28 years); 43.1% of the participants were male. University students were the most targeted population in the found studies (K = 6) and represented 61% of the total population. The NOS was used to assess study quality and risk of bias. Six (K = 6) of the studies had a low risk of bias, whereas four (K = 4) had a moderate risk.
Nomophobia
A random effects meta-analysis of all the available studies evaluated moderate to severe nomophobia in the studies (K = 10, N = 12043). The overall pooled prevalence rate of moderate to severe nomophobia was 63.2% (95% CI: 51.00%-73.86%), with statistically significant evidence of between-study heterogeneity τ2 = 0.63 [0.29; 2.59]; τ = 0.79 [0.54; 1.61]; I2 = 99.3% [99.2%; 99.5%]; H = 12.27 [11.08; 13.60]; 95% PI [19.26%; 86.83%]. Neither age nor sex explained heterogeneity in nomophobia. Detailed results are shown in Table 2.
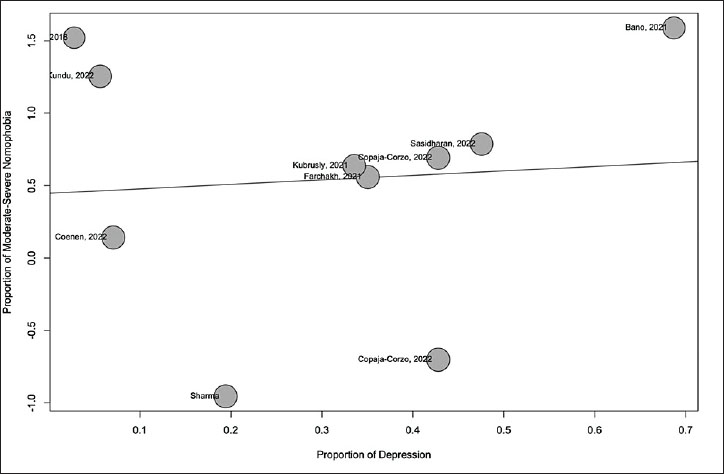
Figure 1. PRISMA 2020 flow diagram for study selection.
Using the NMP-Q to measure Nomophobia, the raw prevalence estimates for moderate to severe nomophobia varied from 28% to 83%. The forest plot of the metaanalysis of nomophobia disturbances in all populations using the NMP-Q is shown in Figure 3.
According to a (leave-one-out) sensitivity analysis, no study had an effect on the global prevalence estimate of more than 2%.
A subgroup analysis of moderate to severe Nomophobia by population was performed. This yielded that the general population and university students scored almost the same prevalence of moderate to severe nomophobia, with the general population being slightly higher, with a prevalence of (K = 3) 67.5% 95% Cl [55.43%; 77.46% ] ô2 = 0.18 ô = 0.43, and (K = 6) 66.6% 95% Cl [48.48%; 80.85% ] ô2 = 0.86; ô = 0.92, respectively. On the other hand, school students scored the lowest prevalence of (K = 1) 27.8% 95% Cl [25.48%; 30.20% ]. A statistically significant difference between populations was observed (p = 0.0001).
Table 1. Chi-square analysis of factors associated with organ donation knowledge.
| SN | Study | Country | Population | Sample (N) | Male:Female | Age (Years) | Tool | Moderate NOM | Severe NOM | Depression cases | NOS (Stars) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Farooqui et al. [19] | India | University students | 145 | 46:54% | 19 | NMP-Q | 87 | 32 | 4 | 6 |
| 2 | Farchakh et al. [8] | Lebanon | General | 2,260 | 41:59% | 28 | NMP-Q | 1,089 | 349 | 792 | 8 |
| 3 | Bano et al. [20] | Saudi Arabia | General | 230 | 47:54% | 22 | NMP-Q | 113 | 78 | 158 | 6 |
| 4 | Copaja-Corzo et al. [21] | Peru | University students | 3,139 | 39:61% | 22 | NMP-Q | 1,052 | 1,040 | 1,343 | 8 |
| 5 | Sharma et al. [10] | India | School students | 1,386 | 67:33% | 16 | NMP-Q | 303 | 82 | 269 | 7 |
| 6 | Kubrusly et al. [22] | Brazil | University students | 292 | 40:60% | 22 | NMP-Q | 156 | 35 | 98 | 8 |
| 7 | Coenen and Grlich [23] | Germany | General | 807 | 10:90% | 25 | NMP-Q | 399 | 33 | 57 | 8 |
| 8 | Copaja-Corzo et al. [24] | Peru | University students | 3,139 | 39:61% | 22 | NMP-Q | 807 | 233 | 1,343 | 8 |
| 9 | Kundu et al. [25] | India | University students | 338 | 50:50% | 21 | NMP-Q | 208 | 55 | 19 | 6 |
| 10 | Sasidharan et al. [26] | India | University students | 307 | 52:48% | NMP-Q | 152 | 59 | 146 | 8 |
Abbreviations: NMP-Q, Nomophobia Questionnaire; NOS, Newcastle-Ottawa Scale.
Notes: K: Represents the number of included studies. N: Represents the number of included samples of the included studies.I2: Refers to the percentage of variation across samples due to heterogeneity rather than chance. ô: Under the presumption that these genuine effect sizes are normally distributed, tau is an estimate of the standard deviation of the distribution of true effect sizes. The prediction interval is computed using tau. ô2: Describes the extent of variation among the effects observed in different samples (between-sample variance). H: Describes confidence intervals of heterogeneity. It is more broadly characterized by the method of moments. As an inherited technique from meta-analysis, it is utilized in meta-regression. Q is Cochran’s Q test, it is non-parametric statistical test to verify whether k treatments have identical effects in the analysis of two way randomized block.
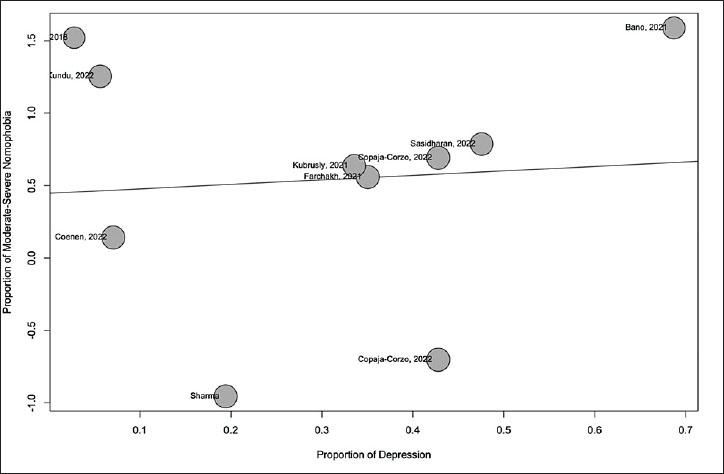
Figure 2. Distribution of studies worldwide.
Depression
A random effects meta-analysis of all the available studies evaluated depression and Nomophobia in the studies (K = 10, N = 12043). The overall pooled prevalence rate of depression was 26.2% (95% CI: 19.37%-34.36%), with statistically significant evidence of between-study heterogeneity τ2 = 0.3653 [0.3521; 3.4753]; τ = 0.6044 [0.5934; 1.8642]; I2 = 98.7% [98.4%; 99.0%; H = 8.93 [7.86; 10.14]. Neither age nor sex explained heterogeneity in depression. The detailed results are shown in Table 2.
Using the DASS-21, HDRS, BDI, and HSCL-25 to measure Nomophobia, the raw prevalence estimates for depression varied from 3% to 69%. The forest plot of the meta-analysis of depression in all populations using DASS-21, HDRS, BDI, and HSCL-25 is shown in Figure 4. The studies by Bano et al. [20] and Sasidharan et al. [26] reported the highest rates of depression at 69% and 48%, respectively.
Table 2. Characteristics of responses.
| Analysis | K | N | Random effects model | Heterogeneity | Moderators | Publication bias | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pooled results [95% CI] | Forest plot | I2 | τ | τ2 | H | Q | Cochran's Q p Valued | Age (Years) | Sex (%Male) | Egger's test | Peter's test | |||
| Nomophobia | ||||||||||||||
| All studies | 10 | 12,043 | 67.44% [51.45%; 59.74%] | Figure 4 | 98.8% | 1.3637 | 1.0526 | 12.27 | 928.96 | 0.001 | - | - | NS | NS |
| University students | 6 | 7,360 | 66.59% [48.48%; 80.85%] | Not Shown | 99.4% | 0.9297 | 0.8643 | - | 862.71 | 0.001 | - | - | NS | NS |
| General population | 3 | 3,297 | 67.44% [55.53%; 77.46%] | 97% | 0.4340 | 0.1883 | - | 65.98 | - | - | NS | NS | ||
| School students | 1 | 1,386 | 27.78% [25.48%; 30.20%] | - | - | - | - | 0 | - | - | NS | NS | ||
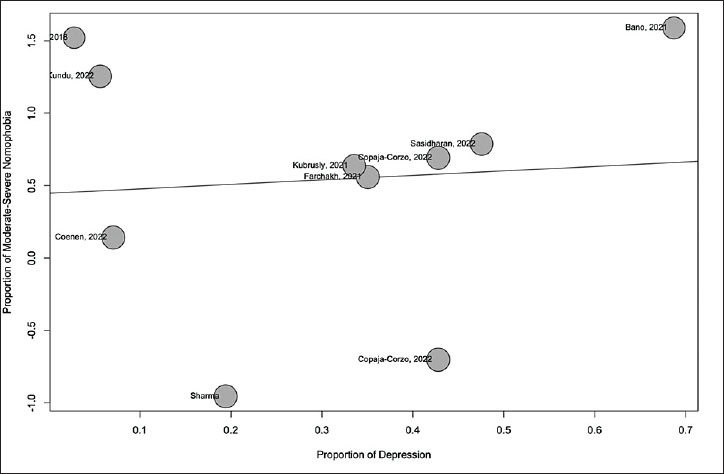
Figure 3. Forest plot of the prevalence of nomophobia.
According to a (leave-one-out) sensitivity analysis, no study had an effect on the global prevalence estimate of more than 1%.
Relationship between moderate to severe nomophobia and depression
A linear regression analysis of Nomophobia and depression yielded no direct linear relationship between the two, as described in the Radial plot Figure 5, and was found to be statistically insignificant (p value = 0.8171).
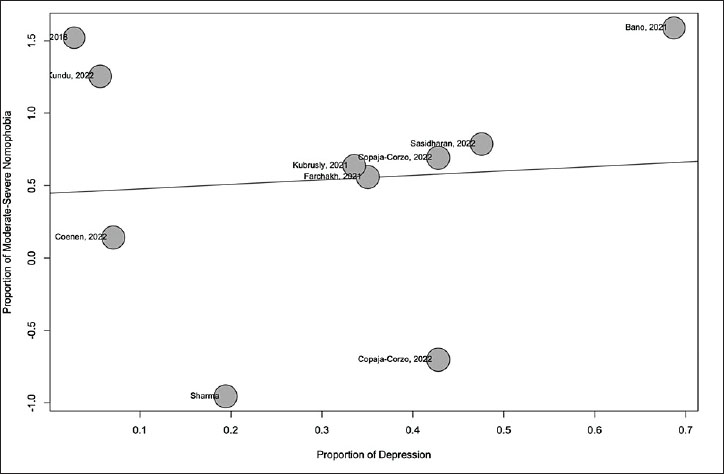
Figure 4. Forest plot of the prevalence of depression.
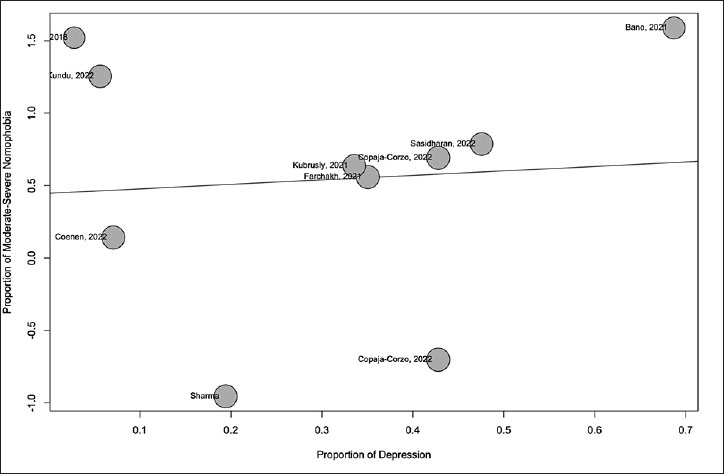
Figure 5. Radial plot of the relationship between depression and nomophobia.
Discussion
This meta-analysis found an estimated pooled prevalence of Nomophobia among the selected studies to be nearly 63%, which is more than the average, with no difference between university students and other populations, and an estimated one in four suffers from depression among the included studies; however, the analysis could not establish a direct association between depression and nomophobia.
As mobile devices have become widely used, people and institutions in the United States and the Western world have gained a greater understanding of the potential consequences of excessive phone usage on mental health and overall well-being [27]. This raised awareness may have prompted proactive initiatives to regulate phone usage and boost healthier connections with technology [27]. This might explain the very few studies reporting nomophobia compared to other countries. Furthermore, mobile phone usage in the United States has been widespread and prevalent for an extended period, with a high level of adoption and extensive utilization for communication, internet access, and various other purposes [27].
In the comparison of the prevalence of nomophobia among different populations, no significant difference was found between populations. Hinting that nomophobia affects everyone depending on different factors, for example, age, type of usage, and amount of usage of mobile phones, as reported in a recent cross-sectional study [24], a recent study suggests that the vast majority of nomophobia occurs among adolescents and those of social media usage.
The reported depression was found to vary widely among studies. This might be possible, as people with preexisting depression are more likely to develop nomophobia as a defense mechanism, as studies have found that excessive smartphone use and nomophobia may contribute to the exacerbation of depressive symptoms. To add more, the self-reported questionnaires used to report depression might have played a role in this variation.
Our study concluded that there is no direct relationship between depression and nomophobia. In an attempt to explain this conclusion, Nomophobia is found to be directly linked to anxiety, which makes it more of an anxiety issue than it is depressive. In recent years, advances in smartphone technologies have caused them to become an indispensable part of human life [28]. Despite their benefits when used for their intended purposes, they still carry a risk of causing various problems for the individual or society when used in a problematic way and excessively [28]. One of these problems is nomophobia [28]. Studies have shown that nomophobia affects all age groups and is very common, especially among the younger generation. In addition, nomophobia carries a threat to both the psychological and physical health of individuals, which raises the importance of raising public awareness about nomophobia and holding seminars in schools, universities, and public services.
Strengths and limitations
This study is the first meta-analysis to specifically examine the independent relationship between nomophobia and depression and was conducted in accordance with PRISMA 2020 guidelines with a large pooled sample. Robust statistical methods, including random-effects modeling and sensitivity analysis, were applied.
However, high heterogeneity was observed, and different instruments were used to assess depression across studies. Most included studies were cross-sectional and relied on self-reported measures, which limits causal interpretation and generalizability.
Conclusion
Based on our meta-analysis, we found no direct connection between depression and nomophobia. However, a more prominent link was discovered between nomophobia and anxiety, suggesting a primary association with anxiety rather than depression. This unique study included all relevant studies, regardless of the scales used, and employed robust statistical modeling to ensure generalizability. This meta-analysis challenges the prevailing belief in a direct link between depression and nomophobia. It emphasizes the complex relationship between mental health and smartphone dependence, offering valuable insights. These findings can pave the way for future research, interventions, and clinical approaches aimed at assisting individuals dealing with nomophobia and related psychological issues.
List of Abbreviations
BDI, Beck depression inventory; CI, Confidence interval; DASS-21, Depression anxiety stress scales-21; HDRS, Hamilton Depression Rating Scale; HSCL-25, Hopkins symptom checklist-25; I2, I-squared statistic; NMP-Q, Nomophobia questionnaire; NOS, Newcastle-Ottawa Scale; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Conflict of interests
The authors declare that there is no conflict of interest regarding the publication of this article.
Funding
None.
Consent to participate
Not applicable.
Ethical approval
Not applicable.
Author details
Khalid M. Alghuthayr1, Rakan H. Hamzah1, Othub S. Albalawi1, Mohammed A. Binjabr1,2, Idrees S. Alalawi1, Fatima A. Hamidaddin1, Saad M. Alotaibi1, Turki M. Alomar1,3, Haitham Jahrami1,4
- Department of Psychiatry, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Bahrain
- King Faisal Specialist Hospital and Research Centre, Riyadh, Saudi Arabia
- Ministry of Health, Riyadh, Saudi Arabia
- Ministry of Health, Manama, Bahrain
Supplementary content (If any) is available online.
References
- Kim JH, Seo M, David P. Alleviating depression only to become problematic mobile phone users: can face-toface communication be the antidote?. Comput Hum Behav. 2015;51:440-7. https://doi.org/10.1016/j.chb.2015.05.030
- Darvishi M, Noori M, Nazer MR, Sheikholeslami S, Karimi E. Investigating different dimensions of nomophobia among medical students: a cross-sectional study. Open Access Maced J Med Sci. 2019;7:573-8. https://doi.org/10.3889/oamjms.2019.138
- King ALS, Valena AM, Nardi AE. Nomophobia: the mobile phone in panic disorder with agoraphobia: reducing phobias or worsening of dependence?. Cogn Behav Neurol. 2010;23:52-4. https://doi.org/10.1097/wnn.0b013e3181b7eabc
- Bhattacharya S, Bashar M, Srivastava A, Singh A. NOMOPHOBIA: No MObile PHone PhoBIA. J Fam Med Prim Care. 2019;8:1297. https://doi.org/10.4103/jfmpc. jfmpc_71_19
- Gonalves S, Dias P, Correia AP. Nomophobia and lifestyle: smartphone use and its relationship to psychopathologies. Comput Hum Behav Rep. 2020;2:100025. https://doi.org/10.1016/j.chbr.2020.100025
- Len-Meja AC, Gutirrez-Ortega M, Serrano-Pintado I, Gonzlez-Cabrera J. A systematic review on nomophobia prevalence: surfacing results and standard guidelines for future research. PLoS One. 2021;16:250509. https://doi.org/10.1371/journal.pone.0250509
- Humood A, Altooq N, Altamimi A, Almoosawi H, Alzafiri M, Bragazzi NL, et al. The prevalence of nomophobia by population and by research tool: a systematic review, meta-analysis, and meta-regression. Psych. 2021;3:249- 58. https://doi.org/10.3390/psych3020019
- Farchakh Y, Hallit R, Akel M, Chalhoub C, Hachem M, Hallit S, et al. Nomophobia in Lebanon: scale validation and association with psychological aspects. PLoS One. 2021;16:249890. https://doi.org/10.1371/journal.pone.0249890
- Jahrami H, Abdelaziz A, Binsanad L, Alhaj OA, Buheji M, Bragazzi NL, et al. The association between symptoms of nomophobia, insomnia and food addiction among young adults: findings of an exploratory cross-sectional survey. Int J Environ Res Public Health. 2021;18:711. https://doi. org/10.3390/ijerph18020711
- Amandeep, Sharma M, Mathur D, Jeenger J. Nomophobia and its relationship with depression, anxiety, and quality of life in adolescents. Ind Psychiatry J. 2019;28:231. https://doi.org/10.4103/ipj.ipj_60_18
- Kuscu TD, Gumustas F, Rodopman Arman A, Goksu M. The relationship between nomophobia and psychiatric symptoms in adolescents. Int J Psychiatry Clin Pract. 2021;25:56-61. https://doi.org/10.1080/13651501.2020.1819334
- Servidio R. Fear of missing out and self-esteem as mediators of the relationship between maximization and problematic smartphone use. Curr Psychol. 2023;42:232- 42. https://doi.org/10.1007/s12144-020-01341-8
- Rodrguez-Garca AM, Moreno-Guerrero AJ, Lpez Belmonte J. Nomophobia: an individuals growing fear of being without a smartphonea systematic literature review. Int J Environ Res Public Health. 2020;17:580. https://doi.org/10.3390/ijerph17020580
- Wolfers LN, Festl R, Utz S. Do smartphones and social network sites become more important when experiencing stress? Results from longitudinal data. Comput Hum Behav. 2020;109:106339. https://doi.org/10.1016/j.chb.2020.106339
- Ahmed S, Pokhrel N, Roy S, Samuel AJ. Impact of nomophobia: a nondrug addiction among students of physiotherapy course using an online cross-sectional survey. Indian J Psychiatry. 2019;61:77-80. https://doi. org/10.4103/psychiatry.indianjpsychiatry_361_18
- Bragazzi NL, Re TS, Zerbetto R. The relationship between nomophobia and maladaptive coping styles in a sample of Italian young adults: insights and implications from a cross-sectional study. JMIR Mental Health. 2019;6:e13154. https://doi.org/10.2196/13154
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88:105906. https://doi.org/10.31222/osf.io/jb4dx
- Luchini C, Stubbs B, Solmi M, Veronese N. Assessing the quality of studies in meta-analyses: advantages and limitations of the Newcastle Ottawa Scale. World J Meta- Anal. 2017;5:80. https://doi.org/10.13105/wjma.v5.i4.80
- Farooqui IA, Pore P, Gothankar J. Nomophobia: an emerging issue in medical institutions?. J Ment Health. 2018;27:438-41. https://doi.org/10.1080/09638237.201 7.1417564
- Bano N, Khan MA, Asif U, Beer JD, Rawass H. Effects of nomophobia on anxiety, stress and depression among Saudi medical students in Jeddah, Saudi Arabia. J Pak Med Assoc. 2020; 70:1-1. https://doi.org/10.47391/jpma.983
- Copaja-Corzo C, Miranda-Chavez B, Vizcarra-Jimnez D, Hueda-Zavaleta M, Rivarola-Hidalgo M, Parihuana- Travezao EG, et al. Sleep disorders and their associated factors during the COVID-19 pandemic: data from Peruvian medical students. Medicina (Mex). 2022;58:1325. https:// doi.org/10.3390/medicina58101325
- Kubrusly M, Silva PGDB, Vasconcelos GVD, Leite EDLG, Santos PDA, Rocha HAL. Nomophobia among medical students and its association with depression, anxiety, stress and academic performance. Rev Bras Educ Md. 2021;45:162. https://doi.org/10.1590/1981- 5271v45.3-20200493.ing
- Coenen M, Grlich Y. Exploring nomophobia with a German adaption of the nomophobia questionnaire (NMP-Q-D). PLoS One. 2022;17:279379. https://doi. org/10.1371/journal.pone.0279379
- Copaja-Corzo C, Aragn-Ayala CJ, Taype-Rondan A. Nomophobia and its associated factors in Peruvian medical students. Int J Environ Res Public Health. 2022;19:5006. https://doi.org/10.3390/ijerph19095006
- Kundu A, Patnaik L, Pattanaik S, Sahu T. Prevalence of nomophobia and use of social networking sites and applications - a cross-sectional study among undergraduate students in a Medical College of Eastern India. J Datta Meghe Inst Med Sci Univ. 2022;17:69-72. https://doi.org/10.4103/jdmimsu.jdmimsu_125_19
- Sasidharan A. Severity of nomophobia and its association with anxiety, stress and depression among medical students during the Covid-19 pandemic. Int J Pharm Res 2022;6:2241-53.
- Jahrami H, Fekih Romdhane F, Pandi-Perumal SR, Bahammam AS, Vitiello MV. Global research evidence on nomophobia during 2008-2022: a bibliometric analysis and review. Psychol Health Med. 2024;29:889-904. https://doi.org/10.1080/13548506.2023.2268888
- Daraj LR, Alghareeb M, Almutawa YM, Trabelsi K, Jahrami H. Systematic review and meta-analysis of the correlation coefficients between nomophobia and anxiety, smartphone addiction, and insomnia symptoms. Healthcare. 2023;11:2066. https://doi.org/10.3390/ healthcare11142066
Keywords: Systematic review and meta-analysis, nomophobia, smartphones, anxiety disorder, depression, moderate to severe nomophobia.

Publication History
Received: January 10, 2026
Revised: February 15, 2026
Accepted: February 17, 2026
Published: March 09, 2026
Authors
Khalid M. Alghuthayr
Department of Psychiatry, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Bahrain.
Rakan H. Hamzah
Department of Psychiatry, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Bahrain.
Othub S. Albalawi
Department of Psychiatry, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Bahrain.
Mohammed A. Binjabr
Department of Psychiatry, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Bahrain.
Idrees S. Alalawi
Department of Psychiatry, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Bahrain
Fatima A. Hamidaddin
Department of Psychiatry, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Bahrain.
Saad M. Alotaibi
Department of Psychiatry, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Bahrain.
Turki M. Alomar
Department of Psychiatry, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Bahrain.
Haitham Jahrami
Department of Psychiatry, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Bahrain.